Health Topics (Sierra Leone)
The Sierra Leone country health profiles provide an overview of the situation and trends of priority health problems and the health systems profile, including a description of institutional frameworks, trends in the national response, key issues and challenges. They promote evidence-based health policymaking through a comprehensive and rigorous analysis of the dynamics of the health situation and health system in the country.
On 30 January 2020, the Director-General of the World Health Organization (WHO) declared the coronavirus disease (COVID-19) outbreak to be a global public health emergency of international concern under the International Health Regulations (2005). Click here for more on WHO African Region numbers at a glance
Sierra Leone update at a glance:
- This is Week 104 of the COVID-19 outbreak in Sierra Leone (Epi week 12 of 2022).
- As of 26th March, 2022, there were 7,674 confirmed COVID-19 cases, 125 deaths and 4,817 recoveries in Sierra Leone
- 347 COVID-19 tests (320 departures, 0 arrivals, 27 suspects) were performed in the last 24 hours in 3 laboratories with a positivity of 0.0%
- There were 0 new COVID-19 cases, 0 recoveries and 0 deaths reported in the last 24 hrs.
- 1 case was reported in SL over the last 7 days compared to 6 cases in the previous 7 days
- 1 of the 16 districts reported COVID-19 cases in the last 7 days Current bed occupancy in COVID-19 community treatment and care centres (CTC/CCC) nationally is 0.0%
- Total COVID 19 tests conducted to date is 338,363 (44.14/1,000)
- Case Fatality Rate (CFR) is 1.6% (excluding community deaths) Nationwide cumulative discharges from quarantine homes are 18,686
- 269 (3.5%) COVID-19 cases are among health workers
- Number of cases in Epi week 11 were 7 compared to 1 in Epi week 10 (600% change). Lab positivity rate for the week increased from 0.03% to 0.20%
- 1,743,563 people (20.5% of total population) had been vaccinated with at least 1st dose of COVID 19 Vaccine in Sierra Leone as at 20 /3/2022.
- 1,125,415 people had been fully vaccinated as at 20 /3/2022 (13.3 % of total population)
Please visit our publication section for more information on the recent COVID-19 situation reports in Sierra Leone
Antimicrobial resistance happens when microorganisms (such as bacteria, fungi, viruses, and parasites) change when they are exposed to antimicrobial drugs such as antibiotics. Microorganisms that develop antimicrobial resistance are sometimes referred to as “superbugs”.
As a result, medicines become ineffective and infections persist in the body, increasing the risk of spread to others.
Why is antimicrobial resistance a concern?
WHO has declared antimicrobial resistance one of the greatest threats to health security today and it is present in every country, including Sierra Leone.
New resistance mechanisms are emerging and spreading globally, threatening our ability to treat common infectious diseases, resulting in prolonged illness, disability, and even death.
Antimicrobial resistance also increases the cost of health care with lengthier stays in hospitals and a need for more intensive care.
What is causing antimicrobial resistance?
Antimicrobial resistance occurs naturally over time, usually through genetic changes. However, the misuse and overuse of antimicrobials such as antibiotics is accelerating this process. In many places, antibiotics are overused and misused in people and animals, and often given without professional oversight.
Lack of awareness among the public, health workers and pharmacists about the appropriate use of antimicrobials also contributes to the issue of resistance in many developing countries.
Examples of misuse include when antibiotics are taken by people with viral infections like colds and flu, and when they are given as growth promoters in animals and fish.
Poor adherence to infection control, especially in healthcare settings, and inadequate sanitary conditions also encourage the spread of antimicrobial resistance.
Current situation
Worldwide, antimicrobial resistance has been reported for key antibiotic and antiviral treatments used for various commonly occurring conditions including pneumonia, bloodstream infections, urinary tract infections, gonorrhoea, tuberculosis, HIV and malaria.
Coordinated action is required to minimize the emergence and spread of antimicrobial resistance. In Sierra Leone, work is progressing towards the development of a national Antimicrobial Resistance Strategic Plan.
WHO is also working closely with the Food and Agriculture Organization of the United Nations (FAO) and the World Organisation for Animal Health (OIE) in a ‘One Health’ approach to promote best practices to avoid the emergence and spread of antibacterial resistance, including optimal use of antibiotics in both humans and animals. With support from USAID, a One Health coordination platform was launched in Sierra Leone in June 2017.
Infection prevention and control
Effective infection prevention and control (IPC) is critical to prevent the spread of antimicrobial resistance.
Worldwide, one in 10 patients acquires an infection while receiving health care. This can contribute to the spread of antimicrobial resistance, with patients requiring subsequent treatments for these infections.
Most of these healthcare-associated infections can be prevented through simple, low-cost IPC interventions performed at critical moments, such as hand hygiene.
The symptoms of cholera include diarrhoea, nausea and vomiting, and severe dehydration. Diarrhoea due to cholera often has a pale, milky appearance that resembles water in which rice has been rinsed, also known as rice-water stool.
The signs and symptoms of cholera in children are similar to adults but they may also experience fever, extreme drowsiness, convulsions or even coma. Only about 1 in 10 infected people develop the typical signs and symptoms of cholera, usually within a few days of infection.
The disease is most common in places with poor sanitation, urbanization, conflict zones and famine. Effective ways to protect yourself include using water that has been boiled, water that has been chemically treated, or bottled water, appropriate use of latrine, regular hand washing.
According to Sierra Leone’s Ministry of Health and Sanitation, Cholera ranks among the five most important epidemic-prone diseases in Sierra Leone. Cholera cases have occurred regularly in some parts of the country with potential of spreading to other areas.
Cholera outbreaks in Sierra Leone
The prevailing strain of cholera in the country is El-Tor which Sierra Leone experienced as its first reported epidemic of the disease in 1970. The outbreak was nationwide, resulting in high incidence and case fatality rate. Since then, the country has experienced a number of epidemics of public health concern, with major outbreaks occurring in 1985, 1994 and 1995. The most recent outbreaks occurred in 2012
In November 2011, the Ministry of Health and Sanitation, through the weekly surveillance reporting system, noted an increase in the number of diarrhoea and vomiting cases. Samples revealed the causative organism as E. coli. In February 2012, the situation worsened and joint assessments were conducted by the Ministry and WHO. Samples collected from Kambia, Port Loko and Pujehun confirmed Vibrio cholera 01 El-tor Ogawa. The Government of Sierra Leone then declared an outbreak of cholera on 27 February 2012. With the onset of the rainy season a further increase in the number of diarrhoea cases was reported in Western Area in week 25 of 2012. Samples collected again confirmed Vibrio cholera O1 Ogawa on 17 July 2012.
As of 31 December 2012, all of the districts except Kailahun were affected with a cumulative total of 22 971 cases and 299 deaths (CFR=1.3%). Western Area which is the most populated district where the capital city is situated reported the highest number of cases (above 50% of the caseload).
Prior to the outbreak, the Ministry had established a National Taskforce on Cholera in April 2011 (comprised of WHO, UNICEF, MSF and Urban WASH Consortium), which developed a preparedness and response plan. The activities of the Urban WASH Consortium were mainly concentrated in Western Urban Area at the time. Following the outbreak the Ministry led the response with the support of partners. This called for a concerted effort to address the epidemic and prevent its spread through effective coordination, surveillance, good case management, prevention, hygiene promotion, communication and social mobilization activities, as well as access to safe water.
As the outbreak progressed, the Ministry with support from partners developed intensified scale-up plans of interventions for outbreak control. On 16 August 2012, the Government of Sierra Leone declared the cholera outbreak as a public health emergency and created a high level multi-sectoral Taskforce. A Cholera Control and Command Centre (C4) was established on the 27 August 2012 to provide coordination and technical advice.
By October 2012, the outbreak was brought under control with the support of multiple local and international partners.
As part of the preparedness and response, a multi-sectoral, multi-year cholera preparedness and response plans are being developed. Meanwhile, cholera is one of the priority diseases listed for daily reporting through the Integrated Disease Surveillance and Response (IDSR) system. The IDSR system also has trained health workers and rolled out community base surveillance to ensure prompt detection and reporting of any major events at the community level.
Ebola virus disease (EVD) is a severe illness that is spread mainly by human-to-human transmission through direct contact with the blood, secretions or other bodily fluids of infected people. EVD can also be transmitted through contact with surfaces and materials, for example clothing and bedding contaminated with these fluids.
The early symptoms of EVD are sudden onset of high-grade fever (38 degrees Celsius and above), fatigue, muscle pain, headache and sore throat. This is followed by vomiting, diarrhoea, rash, symptoms of impaired kidney and liver function, and in some cases, both internal and external bleeding, for example bleeding from the gums and/or blood in the stools.
The most widespread epidemic in history of EVD began in December 2013, and quickly became the most devastating outbreak of the disease since its discovery in 1976.
In May 2014, Sierra Leone had its first case after a woman tested positive upon her return home from a funeral in Guinea. Sierra Leone was one of the countries most affected by EVD with 8,706 people infected by the disease and a total of 3,590 deaths.
WHO declared the EVD outbreak in Sierra Leone officially over on 7 November, 22 months after the outbreak began and 42 days after no further transmissions.
Sierra Leone faced a recent flare-up of EVD in January 2016, however the response was swift and resulted in containment at source as required by the International Health Regulation (IHR 2015). The successful response was attributed to improved preparedness and response capacities combined with prompt detection and strong coordination in legacy of the previous response.
An additional milestone in the effort to defeat Ebola was made on 17 March to mark the end of the flare-up.
At present, the country still remains at risk due to the potential of Ebola virus persistence in the bodily fluids of survivors.
Supportive care-rehydration with oral or intravenous fluids and treatment of specific symptoms, improves survival. Currently, there is no proven treatment available for EVD, however a range of potential treatments including blood products, immune therapies and drug therapies are under evaluation. There are no licensed vaccines available yet, but two potential vaccines are undergoing human safety testing.
|
8,706 Ebola cases in Sierra Leone |
5,116 Ebola discharged cases in Sierra Leone |
3,590 Ebola deaths in Sierra Leone |
More information:
The Government of Sierra Leone Ebola Virus Disease Lessons Learned in Sierra Leone
Ebola outbreak: WHO Current situation update
The WHO is contributing to efforts in strengthening the Sierra Leonean health system by supporting the Ministry of Health and Sanitation (MoHS) in areas such as health workforce planning and management, health information systems, policy and planning, district and hospital management and health financing.
Sierra Leone’s health system is divided into three tiers of service delivery: peripheral health units (PHUs) with extended support provided by community health workers (CHWs); district hospitals; and referral hospitals providing secondary and tertiary patient care. This network of approximately 1,258 health facilities includes 40 hospitals, of which 23 are operated by the government with the remaining owned by private entities and non-governmental and faith based organizations.
The health system is served by roughly 20,000 health workers of different cadres (this does not include CHWs or traditional birth attendants). Some 9 000 of these are volunteers: that is, are not on the government payroll. There are roughly four medical doctors per 100 000 inhabitants and out-of-pocket payments represent 62% of healthcare spending. Since 2010, health services are free for pregnant women and lactating mothers, and children under five years. In terms of health outcomes, the life expectancy in Sierra Leone is 50 years, and maternal and child mortality are among the highest in the world.
The already fragile health system of Sierra Leone suffered a severe shock during the Ebola Virus Disease (EVD) outbreak, with 296 infections among frontline health workers, and 221 recorded health worker deaths. The EVD outbreak was also exacerbated by underinvestment in the country’s health system and a lack of access to affordable health services. With these barriers, many vulnerable segments of the population resorted to alternative treatment methods such as traditional medicines, which also contributed to the spread of the virus.
The Government of Sierra Leone has identified several strategic priorities to address key institutional gaps and strengthen the health system. The Presidential Recovery Plan, launched in mid-2015, focuses on seven priority sectors, including health. Specifically, the plan aims to: 1) save the lives of 600 women and 5 000 children; 2) prevent, detect, respond to epidemics and ensure zero cases of EVD; and 3) ensure continuous care for EVD affected persons and survivors. To achieve this, a Sierra Leone Health Sector Recovery Plan outlines five main pillars: Patient and Health Worker Safety; Health Workforce Development; Essential Health Services; Community Ownership; and Information and Surveillance. These are all priorities for the Government and its partners as the country looks to build a stronger, more resilient health system for its people, and expand access to affordable healthcare.

More information:
Overview of the health workforce 2017
The Government of Sierra Leone Health Sector Annual Performance Report 2015
The Government of Sierra Leone Human Resources for Health Policy (2012), Strategic Plan (2012-2016) and Country Profile (2012)
The Government of Sierra Leone HRH Summit final report
The Government of Sierra Leone Health Sector Operational Plan
WHO Health systems recovery after Ebola
 The Human Immunodeficiency Virus (HIV) belongs to the Retroviridae virus that causes the Acquired Immunodeficiency Syndrome (AIDS). HIV infects protective cells of the immune system, destroying or impairing their function. As the infection progresses, the immune system becomes progressively weak and the individual becomes more susceptible to life threatening opportunistic infections.
The Human Immunodeficiency Virus (HIV) belongs to the Retroviridae virus that causes the Acquired Immunodeficiency Syndrome (AIDS). HIV infects protective cells of the immune system, destroying or impairing their function. As the infection progresses, the immune system becomes progressively weak and the individual becomes more susceptible to life threatening opportunistic infections.
The HIV epidemic in Sierra Leone is considered as mixed, generalized and heterogeneous. HIV affects different population sub-groups and all sectors of the population through multiple and diverse transmission dynamics. The HIV Summary Report for 2015 states that the HIV prevalence in Sierra Leone is 1.25%. The country is rated as one of the least affected compared to others in the sub-region and globally.
The Minister of Health and Sanitation launched the National HIV Strategic Plan 2016-2020 during the World AIDS Day 2015 commemoration in Kenema, Sierra Leone.
The Mode Of Transmission (MOT) identified the population groups with high incidence rates and those at a higher risk of contracting HIV in Sierra Leone. These include fisher folk 10.8%, traders 7.6%, transportation workers 3.5% and mining workers 3.2%. Sex workers, their clients and partners accounted for an estimated 39.7% of new infections, while men having sex with men and Intravenous Drug Users (IDU) have an incidence contribution of 2.4% and 1.4% respectively.
|
50,882 Number of people living with HIV in Sierra Leone in 2015 |
4,398 Children aged 0 to 14 living with HIV in Sierra Leone in 2015 |
30,438 Women aged 15 and up living with HIV in Sierra Leone in 2015 |
|
20,444 Men aged 15 and up living with HIV in Sierra Leone in 2015 |
1.25% Adults aged 15 and up prevalence rate in Sierra Leone in 2015 |
2,505 AIDS related deaths in Sierra Leone in 2015 |
More information:
Sierra Leone HIV Epidemiological Report 2016
HIV/AIDS Strategy for the WHO African Region
WHO Consolidated guidelines on HIV prevention, diagnosis, treatment and care for key populations

Lassa fever is an acute viral hemorrhagic illness caused by Lassa virus, a member of the arenavirus family of viruses carried by the Mastomys rat, found in parts of West Africa. It is considered endemic in Sierra Leone.
Lassa fever can be difficult to detect due to the fact that around 80% of people have no symptoms, or their symptoms are very similar to other prevalent illnesses in the country, for example malaria. These symptoms include fever, fatigue, nausea, vomiting, diarrhoea, headaches, abdominal pains, sore throat and facial swelling.
The Lassa virus is spread to humans from direct contact with infected rats by catching and preparing them for food, or through contact with food or household items contaminated with rat faeces or urine. The virus can also be transmitted through contact with an infected person’s body fluids. People living in rural areas where Mastomys are usually found, especially in communities with poor sanitation or crowded living conditions are at greatest risk.
The lack of resources to invest in diagnostics to easily, accurately and safely test for Lassa fever is a critical issue for early diagnosis and treatment. One in five infections result in severe disease, as the virus affects several organs such as the liver, spleen and kidneys. Many people do not receive the correct treatment, which is why Lassa fever causes so many deaths.
Early supportive care with rehydration and symptomatic treatment improves chances of survival. The anti-viral drug, Ribavirin, has been successful in the treatment of confirmed Lassa cases. It can treat infected people if it is administered as soon as the first signs appear.
Prevention of Lassa fever
Prevention of Lassa fever relies primarily on promoting good “community hygiene” to discourage rodents from entering homes. This includes storage of food in rodent-proof containers, disposal of garbage far from the home, maintaining clean households and keeping cats. Family members should always be careful to avoid contact with blood and body fluids while caring for sick persons.
In health-care settings, staff should always apply standard infection prevention and control precautions when caring for patients. These include basic hand hygiene, respiratory hygiene, use of personal protective equipment (to block splashes or other contact with infected materials), safe injection practices and safe burial practices.
WHO response
The Ministry of Health and Sanitation in Sierra Leone in collaboration with WHO, the Office of United States Foreign Disaster Assistance, the United Nations and other partners have worked together to establish the Mano River Union Lassa Fever Network.
The programme supports countries in developing national prevention strategies and enhancing laboratory diagnostics for Lassa fever and other dangerous diseases. Training in laboratory diagnosis, clinical management, and environmental control is also included.
More information:
Malaria is an acute disease caused by protozoa of the genus Plasmodium, which is transmitted to humans through the bite of an infected female anopheline mosquito. Plasmodium falciparum is the predominant cause of severe malaria in Sierra Leone accounting for more than 90% of all malaria infections. The first symptoms of malaria are headache, fever, joint pains and loss of appetite. They usually appear between 10 and 15 days after the mosquito bite. Without prompt treatment, Plasmodium falciparum malaria can progress to severe illness and death.
Malaria remains a serious public health challenge in Sierra Leone causing immense morbidity and mortality. As one of the biggest killers in the country, malaria is the cause of over 38% of hospital consultations and 17.6% of those admitted then die of the disease. The most vulnerable groups are pregnant women and children under five years old. Malaria transmission is stable all year round in Sierra Leone with peaks at the beginning of the rainy season in May and towards the end of the season in October/November.
Malaria illness shares some symptoms with COVID-19 illness: fever, headache, body aches and weakness. Malaria can coexist with many other infections. Consequently, confirming malaria infection with a diagnostic test does not rule out the possibility that the patient might also be suffering from COVID-19; similarly, testing positive for COVID-19 does not mean that the individual does not also have malaria infection
During the COVID-19 pandemic, the malaria community must remain committed to supporting the prevention of malaria infection, illness and death through preventive and case management services, while maintaining a safe environment for patients, clients and staff.
The Ministry of Health and Sanitation launched the Sierra Leone National Malaria Elimination Strategic Plan (SLNMESP) 2021-2025 in collaboration with Roll Back Malaria partners on World Malaria Day 2021 in Freetown, Sierra Leone.
The Vision: Accelerate the implementation of Malaria Control Interventions towards a Malaria-free Sierra Leone.
Mission: To direct and coordinate efforts towards a malaria-free Sierra Leone through effective partnerships.
Goal: By the end of 2025, contribute significantly to the improvement of the well-being of the population by reducing the malaria burden.
The main malaria prevention and control interventions in the country include: prompt diagnosis and treatment, Long Lasting Insecticide Treated Nets (LLINs), Indoor Residual Spraying (IRS) , Larval Source Management (LSM), Intermittent preventive treatment in pregnancy (IPTp) and in infants (IPTi).
The prevalence rate of malaria in Sierra Leone has decreased from 40% in 2016 to 22% in 2021. By 2025 the Ministry of Health and Sanitation and Roll Back Malaria partners hope to reduce malaria morbidity and mortality by at least 75% compared with 2015.


More information:
The Government of Sierra Leone Malaria Control Strategic Plan (2015-2030)
The Government of Sierra Leone Guidelines for Case Management of Malaria
WHO Global Strategy for Malaria 2016–2030
WHO documents on Eliminating Malaria
The Government of Sierra Leone Insecticide Resistance Monitoring and Management Plan 2016
Prior to the Ebola outbreak, Sierra Leone faced major human resource shortages, well below WHO’s minimum threshold level of 2.28 health care professionals per 1,000. Since 2004, per capita density of doctors, nurses and midwives has fallen below one-sixth of WHO’s recommendations.
At the start of the Ebola outbreak in May 2014, Sierra Leone had one the highest rates of maternal and child mortality globally. The delivery of essential and life-saving care for improved maternal, newborn and child health (MNCH) remains limited due to poor human resources. A severe shortage of trained and supervised health care workforce continues to hamper the provision of MNCH care.
The Ministry of Health and Sanitation (MoHS)has identified underlying reasons causing these capacity gaps: low wages; lack of career advancement; and widespread flaws - opaque practices - governing the recruitment process. Retention of human capital is another challenge identified by the MoHS. Reasons for high turnover include: non-existent incentive schemes for personnel attaining prescribed goals and benchmarks; bottle-necks regarding lack of accountability in staff management; and inadequate mechanisms to cultivate and encourage motivation among care givers.
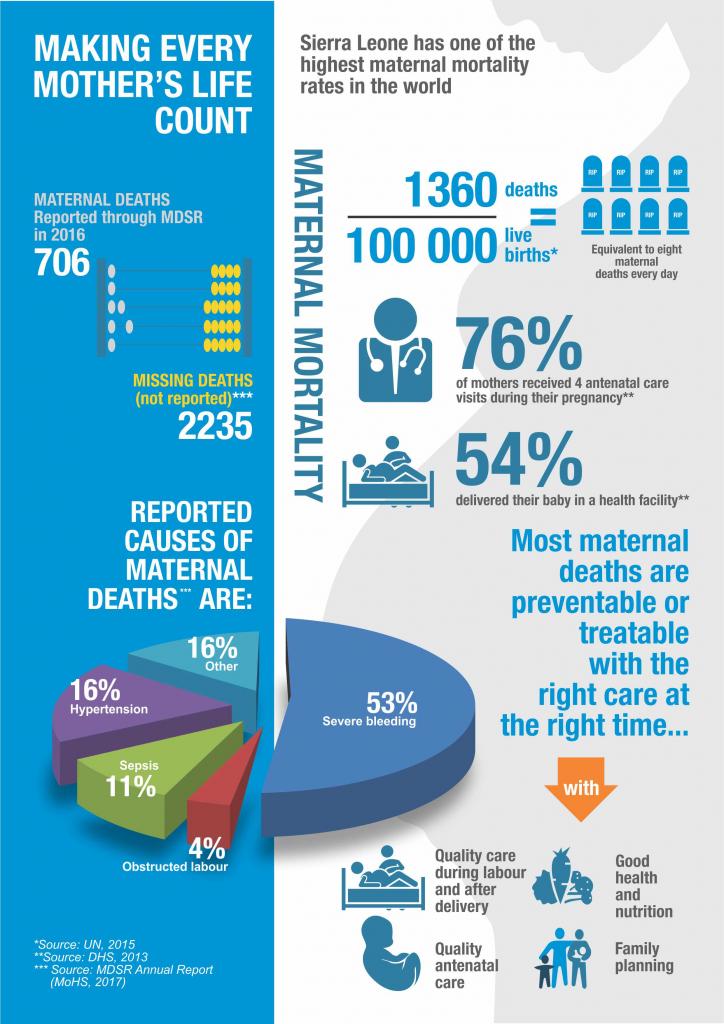
The Government's 2016 Maternal Deaths Surveillance and Response report also makes the following recommendations to addres the country's high rates of maternal deaths: efforts to improve quality of care especially emergency obstetrics, including avilability of key supplies and essantial medicines; promotion of institutional deliveries and antenatal care; access to family planning; timely referrals in the case of complications, and systematic reporting and investigation of all maternal deaths.
In 2010, the Free Health Care Initiative (FHCI) was introduced as a flagship attempt to deliver free preventive and curative health services for pregnant women, lactating mothers and children under five years of age. Whilst this initiative contributed to a some positive MNCH outcomes, its existence remains wholly subject to international support. Since 2014, FHCI remains overshadowed by the Ebola outbreak.
One of the main Ebola to Health transitional priorities in the 10-24 month recovery plan set forth by the President of Sierra Leone in July 2015 is to reduce maternal and child mortality rates by 10%. To this end, the MoHS continues to work with partners to review and streamline existing accreditation mechanisms and improve the quality of education and applied MNCH practices. The Ministry is also spearheading the development and adaptation of evidence based policies, guidelines, and oversight protocols in consultation with international development partners and academic institutions.
|
54% Deliveries take place in a health facility |
87.1/1,000 Estimated infant mortality rate in 2015 |
120.4/1,000 Estimated under-five mortality rate in 2015 |
1360/100,000 Estimated maternal mortality rate in 2015 |
 Download the MDSR Annual Report (2017)
Download the MDSR Annual Report (2017)
Download the infographic (2016)
Making every every mother's life counts 2017 infographic
 Measles is a highly contagious disease caused by a virus in the paramyxovirus family that infects the mucous membranes and then spreads throughout the body. Measles is one of the leading causes of death among young children, and is transmitted via droplets from the nose, mouth or throat of infected persons. The first sign of symptoms is usually a high fever, which appears 10–12 days after exposure to the virus, and then a runny nose, bloodshot eye and tiny white spots on the inside of the mouth can develop in the initial stage. After several days, a rash erupts on the face and upper neck and gradually spreads downwards.
Measles is a highly contagious disease caused by a virus in the paramyxovirus family that infects the mucous membranes and then spreads throughout the body. Measles is one of the leading causes of death among young children, and is transmitted via droplets from the nose, mouth or throat of infected persons. The first sign of symptoms is usually a high fever, which appears 10–12 days after exposure to the virus, and then a runny nose, bloodshot eye and tiny white spots on the inside of the mouth can develop in the initial stage. After several days, a rash erupts on the face and upper neck and gradually spreads downwards.
In Sierra Leone, measles is common and can cause serious complications such as blindness, encephalitis, severe diarrhoea, ear infection and pneumonia among malnourished children and people with reduced immunity.
There is no specific treatment for measles, however Vitamin A supplementation is recommended and treatment of complications as per national guidelines. Most people recover within two to three weeks, and it can be prevented by immunization. Measles immunization in Sierra Leone is given in two doses at nine and 15 months respectively.
A measles outbreak response campaign spearheaded by the Ministry of Health and Sanitation in collaboration with UNICEF and WHO commenced in the Western Area of Sierra Leone on 25 April 2016. The nationwide campaign was launched in response to the measles outbreak that started in the Kono District in August 2015 and later spread to other parts of the country. The majority of victims were under 15 years of age, with a large number under-five thus instigating the decision to target the campaign at children aged six months to less than 15 years old using various strategies including, fixed posts, schools and house to house visits. The second phase of the immunization campaign began on 9 May 2016 to ensure that children in the remaining 12 districts received their vaccine. By 15 May 2016, approximately 2.8 million children aged 6 months to 15 years old in Sierra Leone were vaccinated against the killer disease.
More information:
The Government of Sierra Leone Global Measles and Rubella Strategic Plan 2012-2020

There are many different mental disorders, with different presentations; these include depression, bipolar affective disorder, schizophrenia and other psychoses, dementia, intellectual disabilities and developmental disorders such as autism. Mental disorders are largely characterized by a combination of abnormal thoughts, perceptions, emotions, behaviour and relationships with others. Access to health care and social services capable of providing treatment and social support is key. The burden of mental disorders continues to grow with significant impacts on health and major social, human rights and economic consequences.
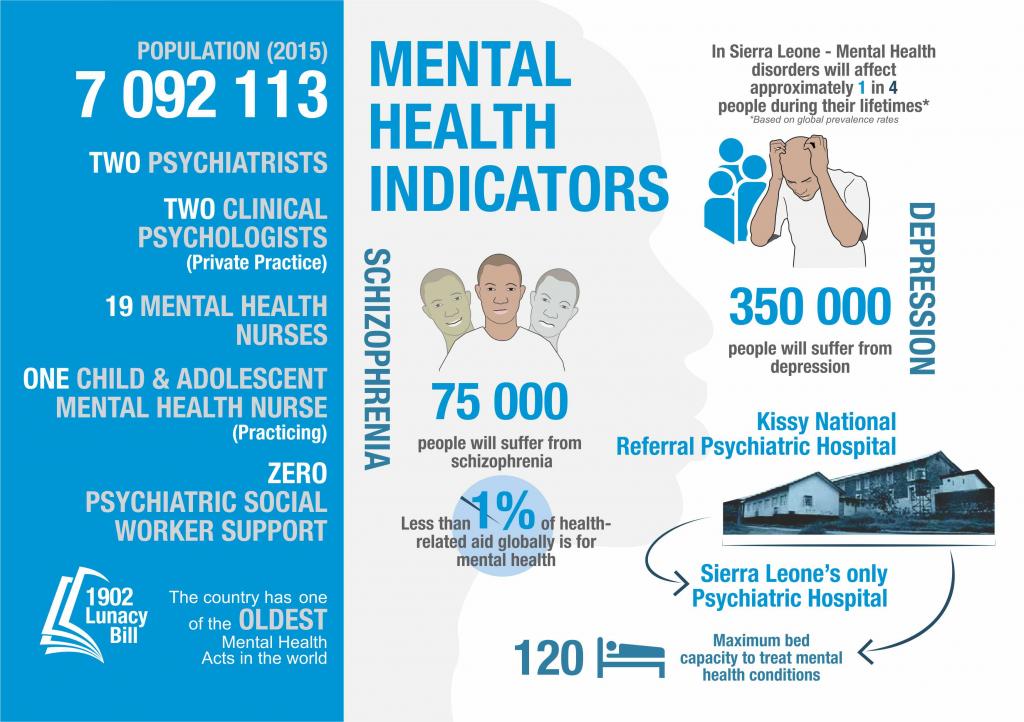
Sierra Leone's mental health legislation, ‘The Lunacy Act’, was written in 1902. The Mental Health Policy expired in 2015, and the Mental Health Strategic Plan requires revision in order to align it to the building of resilient mental health systems countrywide.
Currently, the Sierra Leone Psychiatric Hospital is the only mental health facility in the country, and patients are still chained at this facility. There are three qualified personnel, one Physician, who is the Medical Superintendent, as well as being the National Mental Health Coordinator, the Matron, and one of the In-charges of one of the wards, who is a Mental Health Nurse. The additional staff are Mental Health Nursing Aids who received on-the-job training. Medical treatment is often a last resort in Sierra Leone with most patients being managed “in the Bush” by traditional healers, or spiritual/faith practitioners where patients are also chained.
The country suffers from a severe shortage of trained mental health personnel. There are 19 trained mental health nurses, at least one in each of the 14 Districts who are based at the District Hospital. The majority of those nurses are State Enrolled Community Health Nurse (SECHN) graduates who qualified in 2012 and are the lowest cadre in the nursing establishment of Sierra Leone. There are an additional four nurses trained in Child and Adolescent Psychiatric Nursing, and two of them run the Child and Adolescent Mental Health service at Ola During Children’s Hospital in Freetown.
Mental Health drugs in Sierra Leone are classified as a narcotics, therefore they are difficult to distribute to the Districts and drug shortages are a frequent occurrence.
Efforts to strengthen mental health services in Sierra Leone include psychosocial training for heath workers in health facilities and communities to increase capacity to manage common mental health issues, including through the WHO Mental Health Gap Action Programme and Psychological First Aid.
![]() Download the infographic (2016)
Download the infographic (2016)
Monkeypox is a rare viral zoonosis (a virus transmitted to humans from animals) with symptoms similar but milder from those seen with the now eradicated smallpox disease.
An isolated case of monkeypox was confirmed in Pujehun district, Sierra Leone in April 2017. This was the third known occurrence of monkeypox in the country, with the first reported case in 1970 and the second in 2014.
Monkeypox occurs primarily in the rainforest areas of Central and West Africa. It is transmitted to people mainly from infected animals, including (but not limited to) squirrels, rats, mice and primates. The monkeypox virus has limited secondary spread through human to human transmission; however, it can be transmitted through close contact with an infected person. There is no evidence, to date, that person-to-person transmission alone can sustain monkeypox infections in the human population.
The symptoms of monkeypox include fever, intense headache, lymphadenopathy (swelling of the lymph nodes), back pain, muscle aches and fatigue followed by rash (within 1-3 days after appearance of fever) and then lesions/blisters. The disease is usually self-limiting but needs to be treated in a health facility where symptoms can be managed effectively, and to prevent the spread of the infection.
Case fatality has varied between outbreaks. Typically, it has been between 1 - 10%, with most deaths occurring in younger age groups.
There is no specific vaccine available although prior smallpox vaccination has been shown to be effective in also preventing monkeypox. Preventive measures for monkeypox include hand hygiene and abstaining from trapping and eating bushmeat, especially rodents such as squirrels and rats which are known vectors for the virus.
Health-care workers caring for patients with suspected or confirmed monkeypox virus infection, or handling specimens from them, should implement standard infection control precautions.
Noncommunicable diseases (NCDs) represent a significant burden to Sierra Leone’s already weak national health system. There is a severe lack of of up-to-date information on the prevalence of NCDs such as hypertension, cardiovascular diseases and diabetes. NCDs are estimated to account for 18% of all deaths in Sierra Leone, while the basic capacity of the country to address and respond to NCDs is limited. The last STEPwise approach to Surveillance (STEPS) was conducted in 2009.
Sierra Leone has a huge substance abuse problem where substances such as alcohol, tobacco and sedatives, are widely used. About 90% of admissions to the country’s only psychiatric hospital are due to drug and alcohol related illnesses. Sierra Leone has only three drug rehabilitation centres: two located in Freetown and one in Kenema.
There are four major eye hospitals in the country and training for ophthalmic nurses is provided at the College of Medicine and Allied Health Sciences. However there remains a severe shortage of trained ear, nose and throat (ENT) specialists working in government service and privately run ENT services are out of reach to a vast majority of Sierra Leoneans.
Cancer control is also a significant issue for the country. In 2016, a national assessment of cancer prevention and control including palliative care was undertaken in collaboration with the International Atomic Energy Agency (IAEA), the WHO and the International Agency for Research on Cancer. Three medical personnel were trained on cervical cancer screening and three staff from the Ministry of Health and Sanitation were trained on the prevention and control of cervical cancer. Two sites are also being established for cervical cancer treatment and screening in Makeni and Freetown.
|
Male: 12.7% Use tobacco in Sierra Leone (2015) |
Male: 3.8% Deaths related to tobacco use (2010) |
6.1% of the population Use alcohol |
Male: 5% Obesity rate |
Malnutrition remains an important contributor to under-five morbidity and mortality in Sierra Leone. It places severe burden on the national health system and compromises the growth and development of children, resulting in long term health consequences on the population. While there has been some reduction in malnutrition in the past decade, it still remains a serious problem in most parts of the country.
The Sierra Leone National Nutrition Survey conducted in 2017 indicates that acute malnutrition affects 5.1% of under-fives, 13.6% are underweight while 31.3% are categorized as stunted which according to WHO is high and of public health significance. The survey results also show that exclusive breastfeeding stands at 61.6%, minimum dietary diversity among children 6 – 23 months at 29.7% (based on consumption of four or more food groups) and minimum meal frequency at 44.1%.
Maternal undernutrition is one of the main factors contributing to low birth weight among newborn babies. The 2013 Sierra Leone Demographic Health Survey (SLDHS) report shows that 7% of newborn babies had low birth weight. According to the 2013 Sierra Leone Micronutrient Survey (SLMS) Anaemia among non-pregnant women, pregnant women, and children under-5 stands at 45%, 70% and 76% respectively and 79% of non-pregnant women had folate deficiency which continues to remain a public health concern.
|
31.1% Under-fives affected by chronic malnutrition |
76% Under-fives with Anaemia deficiency |
7% Newborns with low birth weight |
70% Pregnant women with Anaemia |
More information:

Polio is a highly infectious viral disease that attacks the nervous system, and can cause complete paralysis in a matter of hours. The virus is transmitted from person-to-person through ingestion of infected faecal matter. The majority of cases have little or no symptoms whilst the virus is shed intermittently in stools for several weeks following infection. The initial symptoms of polio include fever, fatigue, headache, vomiting, neck stiffness and pain in the limbs.
Since February 2010, Sierra Leone has not recorded a single case of polio. The country is implementing polio eradication strategies including maintaining a high routine oral polio vaccine coverage, conducting supplemental immunization activities and acute flaccid paralysis surveillance.
Sierra Leone joined 154 other countries and territories around the world on 20 April 2016 in the switch from the trivalent Oral Polio Vaccine (tOPV) to the bivalent Oral Polio Vaccine (bOPV) endorsed by the World Health Assembly as a critical component of the polio endgame strategy. In addition, the country is due to introduce Inactivated Polio Vaccine (IPV) into the routine immunization schedule.
More information:
The Government of Sierra Leone Polio Eradication and Endgame Strategic Plan 2013–2018
Rabies virus infects domestic and wild animals and is spread to people through close contact with infected animals’ saliva through bites or scratches.
The main route of rabies transmission to humans is the bite of rabid dogs. Nearly half of those bitten by suspect rabid animals are children aged under 15 years.
There is no reliable data on the burden of human rabies in Sierra Leone. However, the large population of stray dogs particularly in urban communities across the country poses a significant risk factor for transmission of the disease. Meanwhile lack of public awareness about the disease, the need for correct and complete management of animal bites and the scarcity and high cost of the rabies vaccines are some of the major challenges faced in the country.
WHO Expert Consultation on Rabies: first report 2005 [pdf 514kb]
Tuberculosis (TB) is an infectious disease caused by bacteria Mycobacterium tuberculosis that most often affect the lungs. TB is spread from person to person through the air. When people with lung TB cough, sneeze or spit, they propel the TB germs into the air; a person needs to inhale only a few of the germs to become infected.
TB is a poverty disease and the poor and vulnerable suffer the most. Adult men and women in their most productive years are the most affected. The risk of active TB is also greater in persons suffering from other conditions that impair the immune system like HIV, malnutrition, pregnancy and diabetes. TB is often linked to stigma and discrimination which can hinder timely diagnosis and completion of treatment regimes.
Anti-tuberculosis drug resistance threatens the progress that has been made in TB prevention and care. Drug resistance arises when complete treatment is not ensured. Tuberculosis is curable and preventable.
Sierra Leone is among the 30 countries in the world with a high TB burden. The COVID-19 pandemic disrupted access to essential TB services which resulted in reduced TB case detection and impacts on follow-up of patients under treatment.
In 2021, an estimated 24 000 people in Sierra Leone fell ill with TB and more 3 000 died from the disease; 2,800 children became ill with TB; 1 in 4 HIV deaths were due to TB, and an estimated 640 people developed drug-resistant TB (DR-TB).
In March 2017, the MoHS commenced drug-resistant TB case management at a dedicated facility established at the Lakka Government Hospital. Meanwhile since 2016, the MoHS acquired drug-resistant diagnostic capacity with trained staff, using the GeneXpert technology. Presently, 14 GeneXpert sites are providing Drug Resistant TB diagnosis services across the country and Lakka Government Hospital and Makeni regional hospitals are providing MDR-TB treatment services.
TB care and prevention is a priority for the Ministry of Health and Sanitation (MoHS) as formulated in the National TB strategy 2021-2025. Emphasis is laid on improved TB case-finding including in vulnerable groups (children, prisoners, diabetics, miners), addressing the dual epidemic of TB and HIV, addressing drug resistant TB and strengthen community engagement.
In terms of case-finding, 17,669 cases of TB were reported in 2021 and put on treatments from the Ministry of Health and Sanitation’s 184 service delivery points across the country, with a cure rate of 87%. In the same year, the country detected 183 Drug Resistant TB cases and put on second line treatment.
Ending the TB epidemic by 2030 is among the health targets of the UN Sustainable Development Goals adopted in 2015.
|
24,000 Cases in Sierra Leone in 2021 of which 2,800 were children |
298/100,000 Estimated TB incidence in Sierra Leone |
87% Treatment success rate |
 Download the infographic
Download the infographic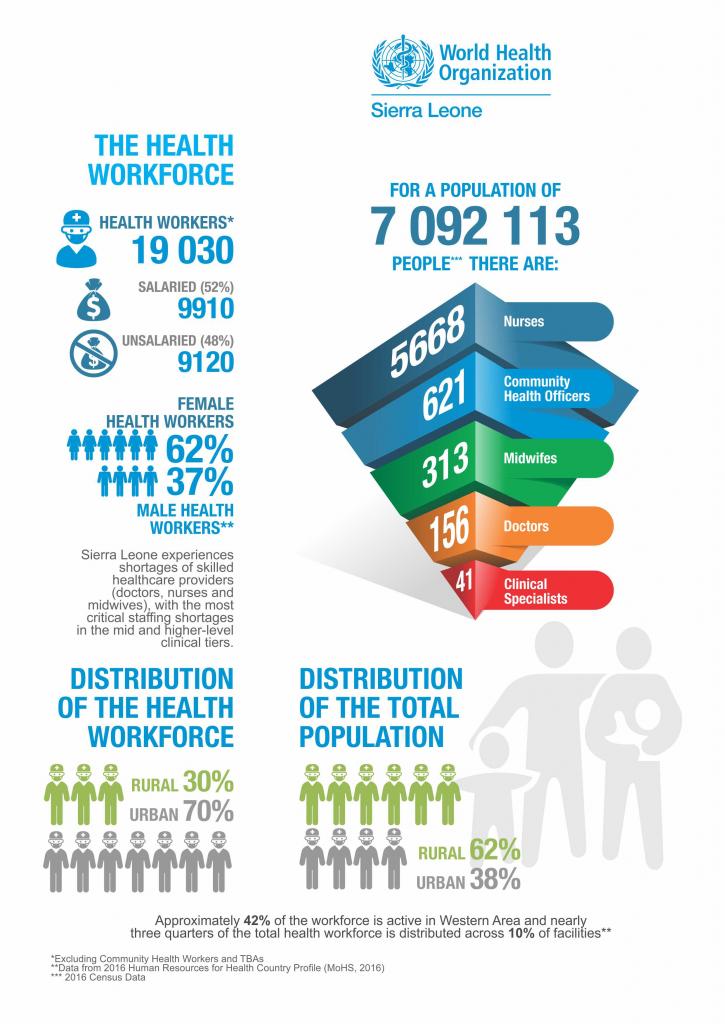{kind=link}
{kind=link}
{kind=link}
{kind=link}
More information:

Yellow fever is a viral disease, found in tropical regions of Africa and the Americas. Sierra Leone has a high risk of yellow fever infection. The disease principally affects humans and monkeys, and is transmitted via the bite of the Aedes mosquitoes. It can produce devastating outbreaks, which can be prevented and controlled by mass vaccination campaigns.
The first symptoms of the disease usually appear three to six days after infection. The first phase is characterized by fever, muscle pain, headache, shivers, loss of appetite, nausea and vomiting. After three to four days, most patients improve and symptoms disappear. However, in a few cases, the disease enters a “toxic” phase in which the fever reappears and the patient develops jaundice and sometimes bleeding, with blood in their vomit. Approximately 50% of patients who enter the toxic phase die within 10–14 days. There is no specific treatment for yellow fever.
On 8 February 2011, Sierra Leone had two cases of yellow fever in Jahun village in Bonthe district, Southern province. A month later the Ministry of Health and Sanitation began a response vaccination campaign targeting 144,479 people aged nine months and above, excluding pregnant women in Bonthe district. Sierra Leone most recently benefited from a yellow fever preventive mass vaccination campaign in 2009, which covered 11 out of 13 districts in the country, excluding Bonthe and Bombali districts.
More information:
WHO Advisory Group on Geographical Yellow Fever Risk Mapping

Zika virus disease is caused by a virus transmitted primarily by Aedes mosquitoes. This is the same mosquito that transmits chikungunya, dengue and yellow fever. Aedes mosquitoes usually bite during the day, peaking early in the morning and late in the evening. Sexual transmission of Zika virus is possible and other modes of transmission such as blood transfusion are being investigated.
The incubation period (the time from exposure to symptoms) of Zika is not clear, but is likely to be a few days. The symptoms are usually mild and last for 2-7 days; these include fever, skin rashes, conjunctivitis, muscle and joint pain, a general feeling of discomfort and headache.
In the past year, Zika has spread throughout South America and thousands of babies in Brazil have been born with a birth defect called microcephaly, where the baby’s head is abnormally small. Guillain-Barré syndrome (GBS) is strongly associated with Zika, however GBS is a rare disorder and only affects a small number of people with recent Zika infection. GBS can cause muscle weakness and paralysis for a few weeks to several months.
As of today there are no cases of Zika in Sierra Leone. A risk assessment was conducted in February 2016 in order to assess each country in the World Health Organization African Region of its likelihood of a Zika virus outbreak and potential of this leading to an epidemic. Sierra Leone was ranked at a medium risk based on a composite index of risk derived from the hazards, vulnerabilities and lacking of coping capacities. In May 2016, local transmission of the disease was reported in Cape Verde. This was the first time that the Zika strain responsible for the outbreaks linked to neurological disorders and microcephaly had been detected in Africa.
There is no specific treatment for Zika, rest, drinking lots of fluids and treating pain and fever with common medicines is recommended. Seeking medical care is advised if symptoms worsen. There is currently no vaccine available.
More information:
The ultimate goal of Infection Prevention and Control (IPC) is to strengthen and standardise the quality and safety of health services for patients, health care workers, and others actors in the health care setting and surrounding environment.
Evidence and lessons gathered from the Ebola outbreak in relation to IPC revealed high vulnerability at every level of health service delivery, including limited awareness of hygiene and infection control procedures among health care providers. This contributed to a high rate of infections among health workers and tragic loss of life.
In response to these issues, Sierra Leone's Ministry of Health and Sanitation established a National Infection Prevention and Control Unit (NIPCU) in 2015 to oversee assessment and implementation of IPC practices in all health facilities.
Nationwide rollout and implementation of National IPC Guidelines, IPC Policy and standardised training began in early 2016. IPC Committees across all structures of the national health system (National Advisory Committee, District IPC Committees and Hospital IPC Committees) are now fully functional.
NIPCU launched a 3-year action plan in November 2016 to build a sustainable and long term programme to monitor and evaluate national level capacity. Monitoring and supervision of healthcare facilities is ongoing to enhance IPC capacity at all levels.
|
28 Number of isolation units across Sierra Leone (2016) |
190 Total bed capacity at Isolation uints across the country (2016) |
8221 Health workers trained on IPC in 2016 |