Ramping up polio outbreak response in southern Africa
Malawi intensifies response after wild poliovirus detected
Lilongwe – Polio emergency response teams in Malawi are ramping up disease surveillance and deepening investigations after the country detected a case of wild poliovirus—the first of its kind in Africa since 2016. Determining the extent of the risk and searching for any further cases are among the crucial steps for an effective response to halt the virus and protect children from its debilitating impact.
The African region was declared and certified as free of indigenous wild polio in August 2020 after eliminating all forms of wild poliovirus. Laboratory analysis linked the strain detected in Malawi to the one circulating in Pakistan’s Sindh Province in 2019.
In January 2022 soon after Malawi received preliminary results of poliovirus, the Ministry of Health, with support from World Health Organization (WHO), swiftly launched response measures, collecting additional stool samples from contacts of the index case, and shipping them for further analysis, as well as actively searching for possible new cases. The country declared an outbreak of wild polio on 17 February following confirmation of the virus type. This is the first case of wild poliovirus in Malawi since 1992.
The African region was declared and certified as free of indigenous wild polio in August 2020 after eliminating all forms of wild poliovirus. Laboratory analysis linked the strain detected in Malawi to the one circulating in Pakistan’s Sindh Province in 2019.
Within days of the outbreak being declared, expert teams deployed to the country to support key response measures including setting up a fully functional environmental surveillance system to complement clinical acute flaccid paralysis surveillance for possible polio cases.
In January 2022 soon after Malawi received preliminary results of poliovirus, the Ministry of Health, with support from World Health Organization (WHO), swiftly launched response measures, collecting additional stool samples from contacts of the index case, and shipping them for further analysis, as well as actively searching for possible new cases. The country declared an outbreak of wild polio on 17 February following confirmation of the virus type. This is the first case of wild poliovirus in Malawi since 1992.
This entails identifying suitable wastewater locations to serve as environmental surveillance sites and training responders at national and local levels to collect and package samples for shipping and analysis.
Environmental surveillance for polioviruses has now been established in six sites in two districts. These include Lilongwe District that encompasses the capital Lilongwe where the initial, and so far the only case, was detected. Other sites are in Blantyre, Mzuzu and Zomba cities.
The polio response teams have also undertaken a risk assessment, which includes detailed disease investigation, epidemiological surveillance assessment as well as analysing factors that can hinder or ease response operations. Additionally, educating and informing the media and the public about polio is ongoing, so they can also report any suspected cases.
To support the country team, experts from the WHO Regional Office for Africa were deployed within days of Malawi declaring the outbreak. The surge team of six includes a coordinator, a technical and operations expert, surveillance experts and a data manager. The WHO team is part of a broader multi-partner Global Polio Eradication Initiative (GPEI) support to the country.
“We have all the necessary tools and all the necessary tactics to successfully stop this outbreak,” said Dr Janet Kayita, acting WHO Representative in Malawi. “Malawi has been polio-free before and can rapidly be so again. The key is to optimize operations and now ensure that every child is reached with the life-saving polio vaccine.”
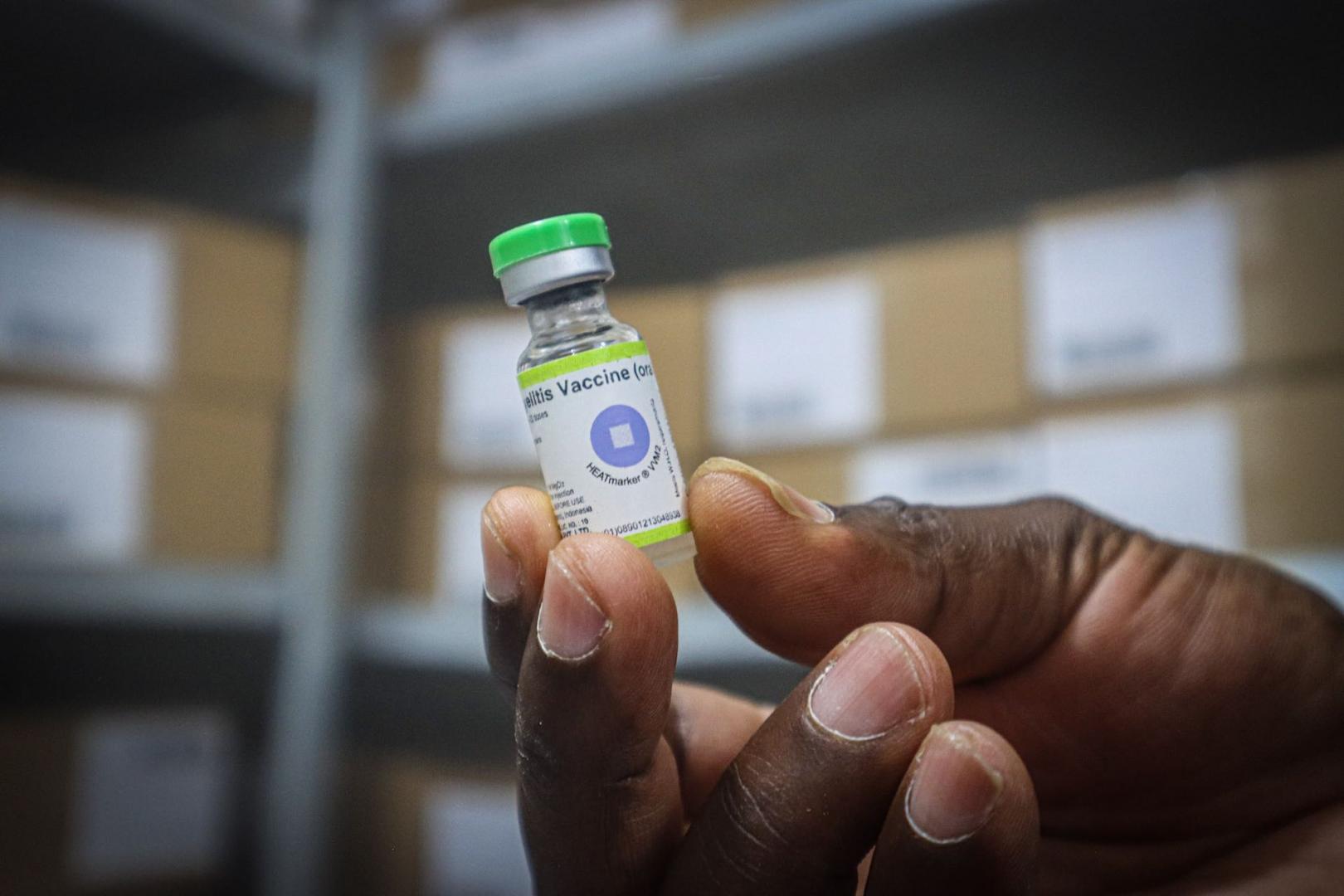
Malawi has scheduled a mass supplemental polio vaccination response targeting under-five children, using the Bivalent Oral Polio Vaccine recommended by WHO and the GPEI partners for wild poliovirus (type 1). Four rounds of polio vaccination campaigns are planned. All the neighbouring countries – Mozambique, Tanzania and Zambia – have been alerted and are planning to conduct immunization campaigns as well.
“The quality of the vaccination campaign is essential to interrupt transmission of poliovirus from child to child. Therefore it is critical to ensure that the vaccination rounds reach every child,” said Deputy Minister of Health, Honourable Enock Phale. “We ask all our political leaders, religious leaders and community leaders to support the government in encouraging our communities to take part in the polio eradication activities by taking their children for the routine polio immunization.”
An immediate-response public awareness campaign has been launched by the Ministry of Health and partners to alert the public of the outbreak, describe the planned response and provide information about polio and the vaccine.
Malawians are treating the outbreak with due urgency.
“I am ready to do whatever it takes to protect my children including getting the polio vaccine. We do not want to see polio paralysing children again as it was 30-plus years ago,” said a resident of Area 24 in Lilongwe, who wished to remain anonymous.
Polio is a highly infectious disease caused by a virus. It invades the nervous system and can cause total paralysis within hours, particularly among children under five. The virus is transmitted from person to person mainly through faecal matter or, less frequently, through contaminated water or food, and multiplies in the intestine. While there is no cure for polio, the disease can be prevented through administration of a safe, simple and effective vaccine.
“Malawi is now considered a polio-affected country. We are working tirelessly with the government and our GPEI partners to reverse this. The WHO African Region’s status as wild polio-free remains intact. However, our work now is to quickly prevent any in-country spread of wild poliovirus and keep children safe,” said Dr Christopher Kamugisha, the GPEI Coordinator.
Zambia’s polio mop-up reaches almost half a million children in 48 hours
Lusaka – Following a Polio outbreak in Malawi earlier this year, frontline health workers in Zambia distributed 4,5 million Oral Polio Vaccines (OPV) to children under five. During the campaign’s last stretch, or ´mop-up´ phase, teams revisited those who were missed, immunising close to 500,000 in the space of two days.
“This is the busiest campaign we’ve had in years. Just yesterday we identified and vaccinated 50 children at an orphanage we couldn’t reach during the main campaign days”, says Vera Shamaya, a nurse for 22 years and Team supervisor at Palabana Clinic in Lusaka’s Chongwe District.
Outside of cities, mop-ups are a race against time to save lives. “We’re so afraid of Polio now. A child who catches it can be paralysed for life and have no future” adds Shamaya. “With mop-ups, we can catch up on vaccinations where we ran out of time or couldn’t get transport”.
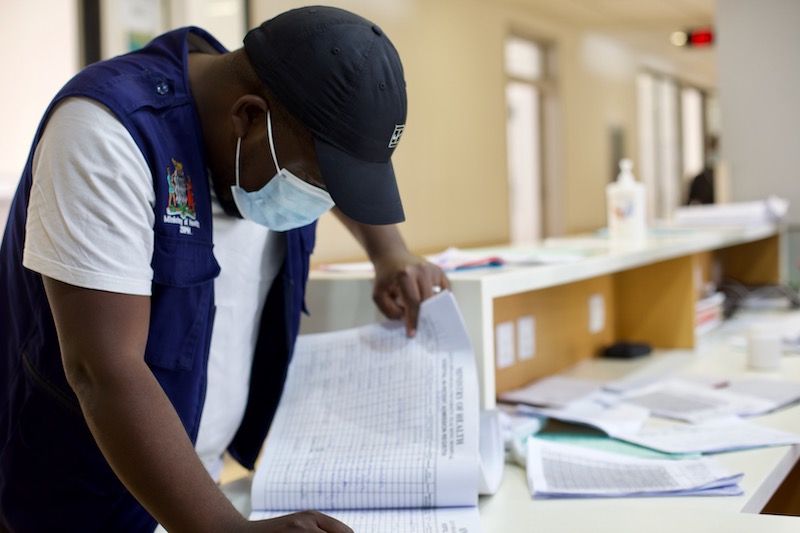
"Independent monitors - professionals from outside the health sector, often teachers or agriculturalists - are essential for casting an objective eye on a campaign’s success."
With the four-day campaign over, it’s time for a two-day nationwide mop-up, a highly critical time for Polio immunisation.
“Our independent monitors have been checking every village in the allocated zone to see if we missed any children,” says Shamaya.
Independent monitors - professionals from outside the health sector, often teachers or agriculturalists - are essential for casting an objective eye on a campaign’s success. They survey every household in a designated area to check if children's nails have been correctly marked after immunization and that the right code is written on their house.
Independent monitors - professionals from outside the health sector, often teachers or agriculturalists - are essential for casting an objective eye on a campaign’s success. They survey every household in a designated area to check if children's nails have been correctly marked after immunization and that the right code is written on their house.
“Where independent monitors fail to see a marker, they report to me and I immediately deploy a team”, says Shamaya. “We’ve just found two children who were missed during the second round and we have to go back”.
A Polio campaign has three phases: pre-campaign, which focuses on preparation and communication; intra-campaign, when key immunisation activities are carried out; and post-campaign, aimed at evaluating the programme. Mop-up is an intra-campaign activity during which teams revisit the homes of missed children.
In this outbreak response, the Global Polio Eradication team opted for a ‘house-to-house’ approach rather than waiting for caregivers to come to a ‘fixed-post’ for vaccination.
While this approach yields high completion rates in densely populated and urban areas, where outreach is fast-paced, it’s another story for the rural landscape.
Zambia has a population density 10 times lower than neighbouring Malawi. In order to leave no child behind, frontline workers sift through every corner of the countryside by motorbike, car or bicycle.
Mable Changala, acting District Health Director in Chongwe says “our designated zone covers facilities as far as 85 kilometres away. Our population is very scattered. Distances are vast, not just between villages, but between each household”. With rural campaigns being so resource intensive, mop-ups are a second chance for meeting vaccination targets.
Dr Barnabas Bessing, Consultant Field Epidemiologist at the World Health Organization, supervises the Polio programme in Lusaka Province. “As a supplementary immunisation activity, the mop-up is one of the pillars of a campaign. It’s an opportunity to analyse setbacks. Children might be hard to reach because of logistics, religious reasons, or conflict. Based on the situation, a mop-up means we can respond with tailored measures,” he says.
Mop-up priority zones also include areas with high population mobility. Should children miss a vaccination round because they are on the farm during the day, mop-up teams will go back in the evening, or for very remote areas, set up camp overnight to see the children early in the morning.

Back at Palabana Clinic, Veria removes an OPV from the freezer for the two missed children identified earlier in the day. Vaccinator Brian and his team have rushed in. Shamaya. briefs them on the location of the household and explains the children were away when they first visited. A short motorbike ride on tarmac and dirt paths later, they reach the family. It turns out it isn’t two but five children who were missed. They vaccinate, record names, mark the children’s fingers and their house.
After checking in on a second family, Brian jumps onto his motorbike. He’s holding down the clutch but the kick-starter he fixed moments earlier has stopped working. “We’ll find a way home,” he says. “All that matters is that we got here”.
A sewage plant, surveillance and polio fight in Zambia
Lusaka – Environmental surveillance teams across Zambia are instrumental to the country’s polio eradication programme. Since the outbreak of wild poliovirus in Malawi in February 2022, they have stepped up efforts for early detection as five countries in south-eastern Africa bolster the drive to vaccinate children and halt the virus.
“My four-year-old son has paralysis due to complications at birth”, says Francis Mbulo, Surveillance Officer at Lusaka Provincial Health Office, “when I do check-ups at children’s hospitals, I can usually distinguish AFP in a heartbeat.”
Acute Flaccid Paralysis, or AFP, presents itself in young children as a weakness in the limbs or neck, facial droop, difficulty swallowing or slurred speech. The syndrome is brought on by a number of causes including severe malaria, meningitis or tick bites. But it’s also one of the key symptoms of poliovirus, which causes paralysis by attacking the central nervous system.
AFP surveillance is the gold standard for poliovirus identification, together with the detection of poliovirus in sewage waters, or environmental surveillance. It is essential to use all the tools in the box. Zambia is stepping up the polio fight as southern African countries ramp up response following an outbreak of wild poliovirus type 1 in Malawi and Mozambique.
“The smell is strong… but you get used to it,” says Mbulo. The team is at Kaunda Square Waste Stabilisation Ponds, which has capacity to treat used waters for over 150 000 Lusaka residents.
The team members wear protective clothing and prepare equipment for a sample collection: a bucket and rope, a bottle, a cooler box with ice packs, a thermometer and disinfectant solution are necessary for the operation.
Mbulo’s team started sampling twice a month in 2019 during an outbreak of vaccine-derived poliovirus type 2. They've now reduced it to once a month as is the standard. Some countries adopt systematic environmental surveillance providing vital information on polio. The more regular the sampling, the more reliable the data.


“Each site has an optimal collection time depending on the sewage flow", says Bornface, one of the surveillance team members.
“At Kaunda square, it's 9.30-10 am”. Collection times are identified by teams from World Health Organisation in Zambia and vary according to proximity of houses and the peak hours of sewage flow. Some sites may also be problematic because of chemical pollution. “We’re particularly careful during the rainy season. The water becomes too diluted so you shouldn’t collect samples if it’s rained in the past hour,” says Bornface.
The sewage water is poured into a bottle which is sealed, disinfected and put into a cooler box destined to the virology lab.
Mobilizing a team of three is essential to avoid cross-contamination. "I collect the sample while Mulenga (another team member) prepares the cooler box and fills in the form", says Bornface.
Bornface and Mulenga both come from Kitwe, an industrial mining town in Zambia’s Copperbelt region. They studied environmental health technology together and are now working together for the polio programme in Lusaka.


"One of the only (few) times we've had a sample rejected was because of a shortage of cooler boxes,” says Mulenga. “That day, we only had one to cover all the sites. As a result of squeezing the four bottles into one box, a leakage occurred during transportation.”
With a Cholera outbreak announced last April, COVID-19, and a number of immunization programmes underway, teams have been competing for resources such as equipment and transport.
Mulenga fills in the environmental surveillance form for the virology laboratory. She notes identification details for the sample such as atmospheric temperature, time and date. The laboratory can tick the ‘poor’ sample box if information on the form doesn't exactly match the bottle.
Mulenga was first deployed to Lusaka for the 2018 cholera outbreak which killed 114 people in Zambia. The district was so affected that health workers were recruited from all over the country.
“It was the most hectic seven months of my life. Cholera spreads so fast that no matter the time, you have to be proactive. I was contact tracing, disinfecting houses, sanitary facilities, and also bodies. The worst was when we lost children. Those memories don't go away,” says Mulenga who now wants to make a difference through the polio programme.


Mulenga fills in the environmental surveillance form for the virology laboratory. She notes identification details for the sample such as atmospheric temperature, time and date. The laboratory can tick the ‘poor’ sample box if information on the form doesn't exactly match the bottle.
Mulenga was first deployed to Lusaka for the 2018 cholera outbreak which killed 114 people in Zambia. The district was so affected that health workers were recruited from all over the country.
“It was the most hectic seven months of my life. Cholera spreads so fast that no matter the time, you have to be proactive. I was contact tracing, disinfecting houses, sanitary facilities, but also bodies. The worst was when we lost children. Those memories don't go away,” says Mulenga who now wants to make a difference through the polio programme.
Nosiku Sitali Muknatu, Environmental Surveillance Technical Supervisor, examines samples. The concentration of poliovirus is lower in environmental sewage than stool samples, but Muknatu is still able to determine the origin of a virus strain as wild or vaccine-derived.
Vaccine-derived poliovirus can occur when a strain of the weakened poliovirus found in the oral polio vaccine changes over time and starts behaving like the wild virus. While it is rare, it is increasingly affecting communities with low immunization rates. The work performed by Muknatu is critical if we are to know which form of the virus is circulating.
The double-pronged approach of AFP and environmental surveillance remains essential to Polio eradication. In Zambia, as of 2018, only 28% of rural households had access to sanitation services and just over half to clean water. And new challenges are yet to come, with climate change already causing water shortages in the country's southern regions.
“I just never want to see children lose their lives to preventable diseases again,” says Mulenga as she leaves the sewage plant, removing her protective clothing and untying her hair.

Deploying data tools in Tanzania’s polio fight
Arusha, Tanzania – Reliable data is crucial for effective disease surveillance and outbreak response. In the wake of the wild poliovirus outbreak in Malawi in February 2022, neighbouring countries stepped up surveillance to detect cases. They have also rolled out mass vaccination campaigns to protect children from the debilitating virus. In Tanzania, the use of Open Data Kit (ODK) tools is accelerating response to alerts of potential polio cases and helping to curb the virus.

“Without the ODK application it would have been way harder to get the early alert we just received,” says Sally Tettey Emmanuel, a WHO Field Epidemiologist on an Acute Flaccid Paralysis (AFP) in Tanzania, referring to a recent alert.
Emmanuel is supporting the national response efforts to fight polio in Tanzania as part of a multi country strategy. Tanzania launched mass vaccination drives in the regions bordering Malawi before expanding across the country to reach all eligible children with the crucial dose. It has already carried out two rounds of polio vaccination.
Emmanuel, working from the Emergency Operations Centre in Tanzania’s northern city of Arusha which was set up with support from WHO, closely monitors every alert and data received via the ODK tool: a fast and effective mobile application that has improved data collection and public health response in the country.
Emmanuel explains how he acted on a recent alert about symptoms of paralysis observed in a child.
“I called the vaccinator that observed the case and headed to the field to conduct the appropriate investigation and sample collection to validate the acute flaccid paralysis (AFP) within 24 hours," Emmanuel says.
AFP is defined by the acute onset of weakness or paralysis with reduced muscle tone in children. There are many infectious and non-infectious causes of AFP. Polio, caused by wild poliovirus (the naturally circulating strain) is one cause of AFP, and so early detection of AFP is critical in containing a potential outbreak. Respiratory and stool samples are optimal for enterovirus detection.
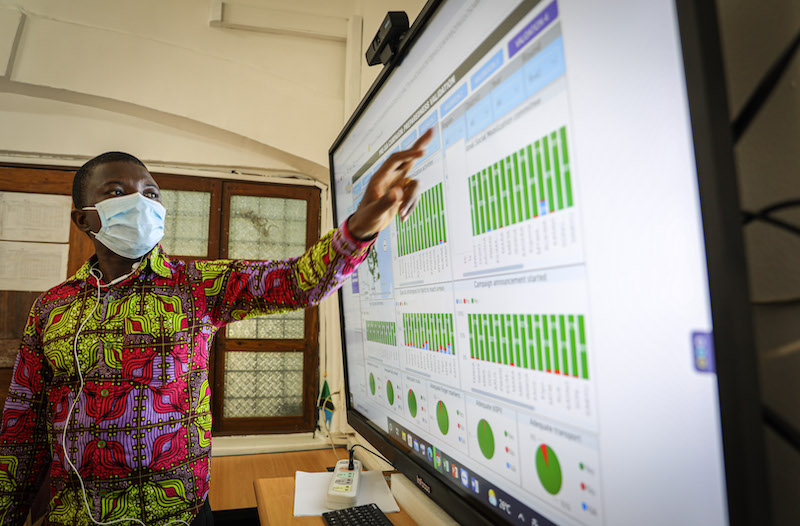
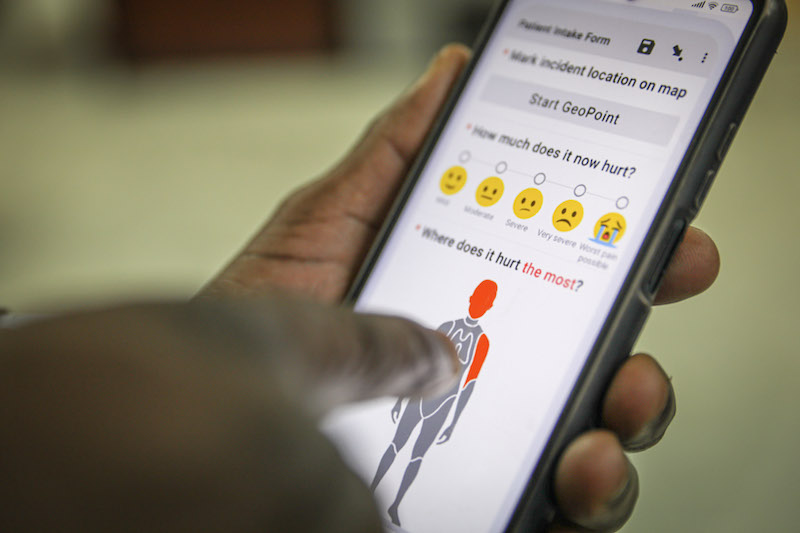
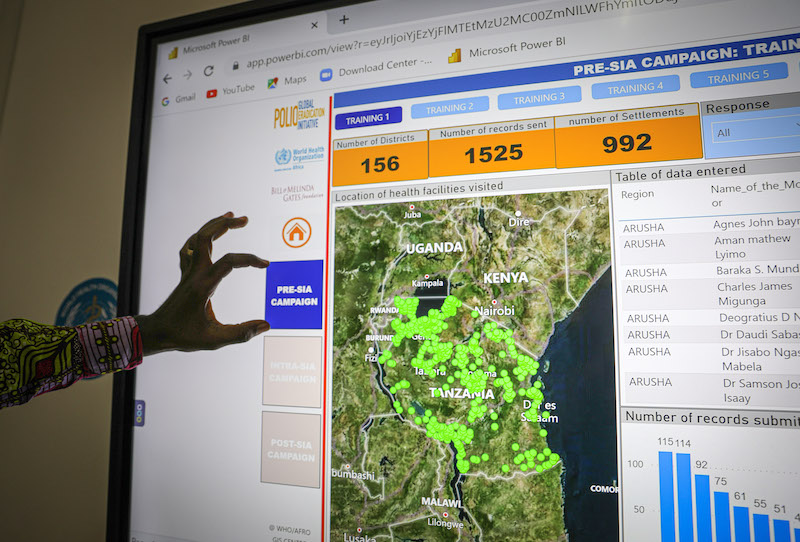
ODK is a simple mobile application that provides software and standards for field electronic data collection. Through a simple editable form, independent monitors, vaccinators, supervisors and health workers can not only plan but also evaluate the quality of a vaccination campaign by logging data and key observations in the forms.
An information dashboard provides near real-time geolocation points (marked using the ODK tool) where vaccination posts can be set up, how many health centres have been visited, the quality of markings on houses visited by vaccinators as well as the quality of finger markers used to identify children who have received the vaccine. ODK also allows to easily determine the location of children who have missed their vaccination.

The results and data from Tanzania’s two wild poliovirus vaccination rounds gathered through the ODK tool will help the health authorities draw lessons and implement the upcoming vaccination phases.
However, the gains of electronic data management are not limited to the fight against polio. Emmanuel notes that with the skills and knowledge acquired in the polio response, he has also been able “to build and introduce similar tools in the routine health care system; specifically, during yellow fever outbreaks or while supporting the tracking of confirmed COVID-19 cases during the pandemic response.”
Media Relations Officer
WHO Regional Office for Africa
Email: dalalm [at] who.int (dalalm[at]who[dot]int)
Tel: +254 703 245 761 (WhatsApp)
Communications and marketing officer
Tel: + 242 06 520 65 65 (WhatsApp)
Email: boakyeagyemangc [at] who.int (boakyeagyemangc[at]who[dot]int)